

Inclisiran: How the NHS became a tool of industrial policy
The Map of Distortion II

I want to show you one node in a project I’m building called The Map of Distortion. It’s a database which tracks pharmaceutical money around the medical industry.
The issue of money in medicine is important, but it’s complex and difficult to grasp intuitively. To unpack this problem, I’ll show you the pathway of one drug, from its discovery all the way through to its delivery in a hospital. That way, you’ll see how each node it passes through distorts reality before it finally ends up in your prescription.

The drug we’re going to look at is a cholesterol-lowering drug called inclisiran. To really understand it, we must first understand the market at which this drug is aimed; the statin market in the UK, Europe and USA is huge and this behemoth market has been created almost entirely by the pharmaceutical industry itself. What started out as a targeted drug for high-risk cardiac patients has been aggressively engineered into a “mandatory mint” for millions of perfectly healthy adults. So this is what we must remember: our “inclisiran” drug, is creation of the pharma industry, and it aims to service a huge market created by the pharma industry.
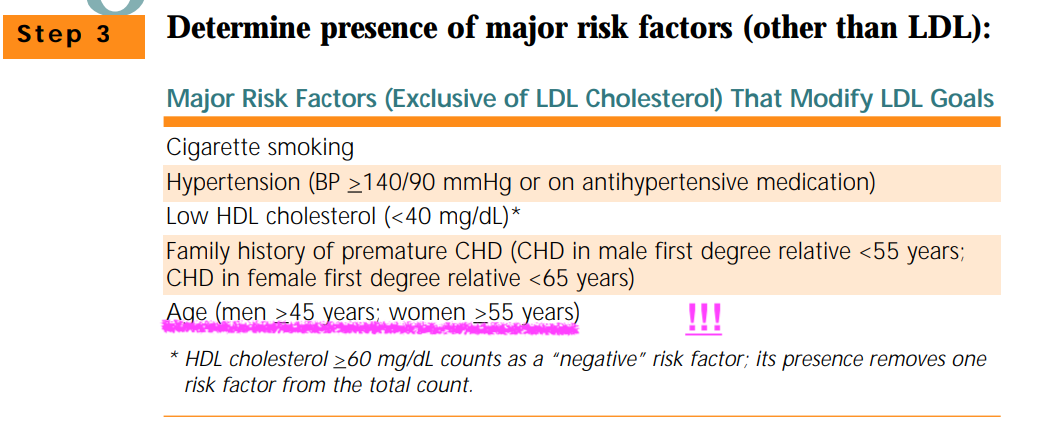
How do you ‘create’ a market for a drug exactly? You spend decades lobbying to systematically lower the clinical thresholds for “high” cholesterol to such low levels that millions of healthy people become ‘sick’ according to your new criteria. That’s how. Critics will argue this is a cynical view, but consider this: if you’re a male over the age of 45, in America you’re considered high risk by default. For women, the high risk group is over 55. We’re talking about maybe 40% of the entire US population become eligible for the drug.
In the UK, at 45 if you get your cholesterol checked, there’s a very good chance you’ll be recommended statins. Nothing else about your lifestyle or health really matters according to these guidelines. From a financial perspective, creating a market this large this is a remarkable achievement, so how did they do it?
The systematic lowering of clinical treatment thresholds got started (as it often does) in the United States. The 2004 National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) guidelines was the blueprint used to expand the market for statins. These guidelines lowered the recommended LDL-Cholesterol targets across a range of high risk categories, which immediately classified millions of healthy individuals as “high risk” and therefore eligible for statin drug therapy.At the wave of a pen, the market size increased massively.
So was the process by which this happened fair? Well, eight of the nine members of that NCEP ATP III panel had direct, personal financial ties to the manufacturers of statins. Furthermore, the five major clinical trials used to justify the new guidelines were entirely funded by the pharmaceutical companies that manufactured the drugs. A majority of the principal investigators involved in those trials had received substantial financial compensation from the sponsors through consultancies, lecture fees, or direct employment.
The pattern repeated itself in 2013. This time the guidelines came from the American Heart Association and the American College of Cardiology, and they pushed the eligible population wider still — recommending statins for an estimated 31 million more Americans on top of the 25 million already taking them. And when the British Medical Journal looked at who had written them, it found the same fingerprints all over again. Eight of the fifteen panel members had financial ties to industry, and the chair himself, Professor Neil Stone, had been paid by six different statin manufacturers in the years before he took the role:
“Stone (on the panel) acknowledged to the BMJ that before being empanelled he had financial ties to Abbott, AstraZeneca, Merck, Pfizer, Sanofi-Aventis, and Schering-Plough, and he had served as a consultant to Abbott, AstraZeneca, Merck, Pfizer, Reliant, Schering-Plough, and Sonaste. All six corporations to which Stone had financial ties make drugs to treat hyperlipidemia…
Six of the remaining panelists also disclosed ongoing financial ties to drug makers during their service on the panel.“
British Medical Journal, 2013
These guidelines, heavily influenced by industry money, kick started the trend that pure demography could be used to determine cardiovascular risk factors. The result? Men aged 45 or older became a high-risk cohort by default. This single act successfully transformed healthy, aging males into a permanent consumer base.
The trend arrives in the UK
Following the global precedent set by the US guidelines, the United Kingdom followed suit and expanded its own market. The industry wanted more people eligible for statin prescriptions, so that’s what we got.
The National Institute for Health and Care Excellence (NICE) recommended starting statins only in individuals with a 10-year cardiovascular disease risk of more than 20%. In July 2014, NICE issued Clinical Guideline 181, which halved this treatment threshold to a 10-year risk of more than 10%. There’s a pattern here which will become obvious...On the panel making these recommendations, 8 of the 12 members had financial ties to drug firms making statins. According to my own Map of Distortion, I found three of those members now direct pharmaceutical consultancies, whilst another three declare payments from pharma giants.
This guideline change generated widespread controversy within the UK medical community. A survey conducted by Pulse revealed that 57% of general practitioners (GPs) did not support the draft guidance, and 55% stated they would refuse to take a statin themselves or recommend it to a family member at the 10% risk threshold. Despite the professional backlash, the guideline was implemented, making more than 80% of men over 50 and half of women over 60 eligible for statin therapy.
The chicanery has bloated this global market into a mammoth $17.1 billion, anchored by more than 200 million annual prescriptions dispensed annually in the US alone. There are only 342 million people in the United States, so this is an incredibly high number of annual prescriptions. It’s into this market, artificially inflated and eye-wateringly lucrative, that the drug we’re now going to track, inclisiran, makes its debut.
The Birth of our drug
Unlike the daily tablet form of statins, Inclisiran it’s a twice-a-year injection that aims to lower your cholesterol. Why would a company like this injection format? Well, statins as drug ‘type’ go stale because financially - as a category - statins have already been juiced. Prior to its patent expiring in 2012, Lipitor (a statin) became the highest grossing drug in history, raking in at least $130 billion over its lifetime. But all great things must come to an end, because in 2012 the patent for the drug expired. UK doctors can, and do, prescribe generic versions of the drug for as little as 9 pence a tablet.
So the job is done right? Maybe cholesterol is a cause of heart disease, and if required, we can moderate cholesterol cheaply and effectively with post-patent generic drugs based on Lipitor?
Well...yes and no, because the pharmaceutical industry hate patent expiry. Having worked very hard to create the market (by lowering the threshold for ‘high’ cholesterol), they can’t just allow their cash-cow to be killed by patent expiry. The industry have a well trodden solution to this annoying problem. They invent brand new ways to lower cholesterol, then they lobby and market their new (ownable) versions to health systems around the world. Why spend pennies per treatment when there’s a better (and more expensive) treatment now on the market!?
It’s in that spirit, that the twice-a-year injection of Inclisiran is conjured into existence. Let’s skip to the end of this story shall we? By 2021, the NHS agreed to roll it out to as many as 300,000 people in one of the biggest medicine deals in its history. Remarkably, it did so before the trial investigating if the inclisiran actually prevents heart attacks, strokes or deaths was published. As I write, that study still hasn’t been published.
So how on earth does all this happen?
It starts, like a lot of these, with public science.
Inclisiran is built on a piece of Nobel-winning biology — RNA interference, the trick of switching a gene’s messaging off. That science was done between 1998 and 2006 in the United States, Canada, and Germany. Most of this work, as far as I am able to tell, was funded by grants from NIH, Canada’s CIHR and the Max Planck institute. Researchers worked out they could use this RNAi technology to lower the production of PCSK9 proteins in the body, which ultimately lowers your cholesterol.
This whole process was turned into a drug platform by a biotech company called Alnylam. From there, the ‘cholesterol lowering’ gene moderation was named ‘inclisiran’ and licensed to a company called The Medicines Company, which paid for this new drug to go through medical trials. The initial results were made available in 2019, and a little over eight days later (before the first trial was even peer reviewed) Novartis bought the company for around $9.7 billion. Clearly, they must have had their eyes and ears closely on that drug, because at that price, they clearly believed it could be a blockbuster.
The first study (Orion-10) was properly published in New England Journal of Medicine a few months later in 2020. It’s possible to check the study’s declared interests and it’s an incredible demonstration of just how conflicted by pharmaceutical cash a study can actually be. In the declared interests section, it’s hard to find an author without a massive, at times almost laughable connection to the industry.
This study was paid for by the Medicines Company, the company that owned the drug. Of the 11 authors in the study, every single one of them had a direct paid relationship with that company. In some cases, they happily declared “employment, shares and stock options” in the very product they’re studying. Even more strange is the sheer scale at which some of these people take personal fees from the industry. The most bizarre component? This is completely normal. This is how medical science is done; in a pressure cooker of corporate money, special interests and conflicting funding. Given that every single person in the study stood to benefit from a positive result, what result do you think emerged from the study?
Dr. Ray reports receiving lecture fees from Aegerion Pharmaceuticals, Kowa, Cipla, Algorithm, and Zuelling Pharma, grant support, paid to his institution, lecture fees, and advisory board fees from Amgen, Regeneron Pharmaceuticals/Sanofi, and Pfizer, lecture fees and fees for serving on steering committees for trials from AstraZeneca and Eli Lilly, fees for serving on steering committees for trials from Cerenis Therapeutics, the Medicines Company, and Esperion, advisory board fees from Akcea Therapeutics, Novartis, Silence Therapeutics, Bayer, and Daiichi Sankyo, lecture fees and advisory board fees from Takeda, Boehringer Ingelheim,
Dr. Reddy’s Laboratories, grant support and advisory board fees from Merck Sharp & Dohme, fees for serving on a clinical events adjudication committee from AbbVie, and fees for serving as principal investigator for a trial from Resverlogix;
Dr. Wright, receiving advisory board fees from Sanofi and Regeneron Pharmaceuticals, consulting fees from Gilead Sciences, and fees for serving on a steering committee from AstraZeneca;
Dr. Kallend, being employed by and holding stock options in the Medicines Company; Dr. Koenig, receiving consulting fees and lecture fees from AstraZeneca, consulting fees from Novartis, Pfizer, the Medicines Company, DalCor Pharmaceuticals, Kowa, Amgen, Corvidia Therapeutics, and Daiichi Sankyo, lecture fees from Berlin-Chemie and Sanofi, and grant support and provision of reagents from Singulex, Abbott, Roche Diagnostics, and Dr. Beckmann Pharma;
Dr. Leiter, receiving grant support, paid to his institution, advisory board fees, and fees for CME from Amgen, Eli Lilly, and Regeneron Pharmaceuticals/Sanofi, fees for serving on a steering committee from Esperion, grant support, paid to his institution, and fees for serving on a steering committee from Kowa and the Medicines Company, advisory board fees and fees for CME from Merck, and advisory board fees from HLS Therapeutics;
Dr. Raal, receiving advisory board fees and lecture fees from Amgen, Sanofi-Aventis, Regeneron Pharmaceuticals, and the Medicines Company;
Ms. Bisch and Ms. Richardson, being employed by and holding shares and stock options in the Medicines Company;
Dr. Jaros, receiving fees for providing statistical analysis for trials from the Medicines Company;
Dr. Wijngaard, being employed by and holding shares and stock options in the Medicines Company;
Dr. Kastelein, receiving consulting fees from Akcea Therapeutics, AstraZeneca, CiVi Biopharma, Corvidia Therapeutics, CSL Behring, Daiichi Sankyo, Draupnir Bio, Esperion, Gemphire Therapeutics, Madrigal Pharmaceuticals, Matinas BioPharma, NorthSea Therapeutics, Novo Nordisk, Novartis, Regeneron Pharamaceuticals, REGENXBIO, Staten Biotechnology, and 89bio. No other potential conflict of interest relevant to this article was reported.
The trial that actually matters, ORION-4, is the one testing whether inclisiran actually prevents heart attacks and strokes. It’s run out of Oxford’s Clinical Trial Service Unit, and it’s co-sponsored by the University of Oxford and Novartis itself. That’s worth sitting with; the supposedly independent trial that will tell us whether this drug saves a single life is also co-funded by the company that sells it. And, the University that runs the study, according to preliminary data in the Map of Distortion, took £16 million in pharma money between 2019 and 2024. According to the Map of Distortion, Oxford’s single biggest pharma funder? Novartis, at around £9 million.
So… although it’s conflicted massively by money from companies which stood to benefit, there’s now a handful of studies which show the drug can lower cholesterol. Even without data to show it has any real clinical health benefit, is it possible to get this thing onto the market? Of course it is. Here’s how.
On the market with incomplete data
To get a drug onto the UK market, you have to take it to the MHRA, which is the UK’s drug regulator. Long time readers of The Digger will know that the MHRA isn’t funded by the taxpayer. If it isn’t funded by the taxpayer, then who is it protecting?
To get a drug onto the UK market, you have to take it to the MHRA, the UK’s drug regulator. Long-time readers of The Digger will know the MHRA isn’t funded by the taxpayer. And if it isn’t funded by the taxpayer, then who is it really protecting?
If you can believe it, the MHRA is mostly funded by the very industry it’s supposed to be regulating. This is like the mafia paying for the city’s police, or arms dealers bankrolling the war-crimes tribunal. The MHRA’s job is to license a pharmaceutical product for use in the UK, and it takes 86% of its funding from the very industry that wants every single one of its products on the market. A 2022 investigation in the BMJ put it bluntly, quoting the sociologist Donald Light: drug regulators have become “a prime example of institutional corruption”
I’d agree with that — but I think it gets worse. It’s almost impossible to find out how the drug was actually assessed. I went looking for the UK assessment of inclisiran — who reviewed the data, who decided it was safe for the UK market, what they declared — and on the UK side, I couldn’t find it. The MHRA used to lean on the European Medicines Agency to assess drugs like this, and an FOI request simply points you back to Europe.
Remarkably, the MHRA states that the contents of its own reports on inclisiran “are confidential on the grounds that it is comprised of information supplied in confidence in the form of European assessment reports which are not available in the public domain.”
That’s worth pausing on, because the European regulator does publish a public assessment report for inclisiran — I downloaded it, all 143 pages of it. A fuller version, with the commercially sensitive detail stripped out, is kept confidential, and that may be what the MHRA is leaning on. But the public report alone is revealing — and the UK regulator points you away from its own reasoning entirely, telling you to go and read Europe’s.
And what did Europe’s regulator actually conclude? In its own assessment report, it approved inclisiran while admitting, in black and white, that “a limitation of the dossier is the lack of cardiovascular outcome data” — that the cholesterol drop is “only a... surrogate,” and that “a favourable impact on CV outcomes has not yet been confirmed.” To translate: we don’t have the data to say this prevents a single heart attack or stroke — but we’re letting it onto the market anyway
So if we can’t see into the MHRA’s reasoning, what can we do? The MHRA takes its expert advice from a standing body called the Commission on Human Medicines, and a drug like inclisiran would fall under its remit. I can’t prove which of these specific people assessed this specific drug — that’s exactly the problem — but I can tell you who sat on that Commission in the year inclisiran was waved through, and, to some degree, what they had declared. Of its fourteen members, nine declared a financial interest in the pharmaceutical industry. Two of them, including the Commission’s own chair, Professor Sir Munir Pirmohamed, declared a tie to Novartis, the maker of the drug which was waved through.
Shall we recap? The science was publicly funded, and the profits were taken private. The drug went to The Medicines Company, which ran the trials with investigators on its own payroll and published only preliminary surrogate data — a fall in cholesterol, with no evidence it prevents a single heart attack — and Novartis bought the whole company anyway. The one trial designed to find a real clinical answer is run out of a Novartis-sponsored Oxford University, and won’t report for years. The drug was then taken to a UK regulator that draws 86% of its funding from the industry it polices, where the assessment vanishes into a grey box that’s almost impossible to audit — overseen by an expert committee on which a large share of the members have serious ties to that same industry.
It’s getting silly, but we’re not done. Getting onto the market is only one battle. To reach the bedside, you need a recommendation — and in the UK, that’s where NICE comes in.
The experts who vouched for it were paid by the company that makes it.
As I explained last time, NICE run ‘Technology Appraisals’ for new drugs hoping to get a recommendation at the NHS level. When NICE appraised inclisiran, it invited expert advisers into the room and published what they’d declared. The lead clinical expert was Professor Kausik Ray of Imperial College London — who is also the lead investigator of the ORION Inclisiran trials, and in his own declaration, “a consultant to Novartis.”
I ran his name through the drug industry’s own UK payments database to confirm this. It records hundreds of thousands of pounds in payments paid to Professor Ray by Novartis — the maker of the drug he was advising on. In The Map of Distortion database, which collates data no longer published by Disclosure UK, we see that Professor Ray has received more than £570,000 from drug companies over the six years of data it has collected.
I will stress, Professor Ray has done nothing illegal or wrong here. He declared his financial ties, NICE recorded it, and decided his ties “would not prevent Professor Ray from providing expert advice to the committee.”
Also in attendance was Dr Alan Jones, a Principal Investigator at the Oxford University trial of inclisiran. He’s the local principal investigator on a Novartis-funded trial of inclisiran — running it at his hospital — while advising NICE on whether the NHS should pay for that very same drug. NICE’s conclusion on this conflict of interest? It “would not prevent Dr Jones from participating in discussions on this appraisal”
Also in the committee was a patient expert from HEART UK, the cholesterol charity. Heart UK had just begun working with Novartis and they’d recently held a conference, which Novartis sponsored. According to The Map of Distortion, in the year inclisiran was appraised, HEART UK took nearly £59,000 in donations from Novartis. What was the upshot of this? The declaration would not prevent this person “from providing expert advice to the committee.”
If this is getting exhausting, please hold on because we’re not done here. Inclisiran was appraised by the somewhat permanent NICE Committee C. The current chair of that committee, Dr James Fotheringham has declared paid Novartis consultancy and speaker fees (TA723, TA751, TA853) and according one other declaration, his employer (The University of Sheffield), also took Novartis funding (TA706). According to my own (preliminary) results in The Map of Distortion, Fotheringham took £3,433 from Novartis across 2020 and 2021, and the University he works for had a good year in 2020, taking £51,532 from Novartis.
Also on that committee sits Dr Richard Nicholas. In fact, he’s vice-chair of the committee. He declares paid Novartis & Roche advisory boards across more than 20 other technical assessments. Disclosure UK corroborates this with a payment of £4,452 in 2022.
So...What do you think the outcome of the appraisal was?
They recommended it of course! In October 2021, NICE approved inclisiran for the NHS — waved through on the strength of how much it lowers cholesterol, just a number on a chart, while the ORION-4 trial Dr Jones was running was still years from reporting if the drug prevents even a single heart attack or stroke. Five years later, that study still hasn’t reported that data. We’re expecting to maybe hear something in July.
So the drug’s own trial investigators, at least one definitely paid by Novartis, spoke in its favour; the patient voice was funded by Novartis; the committee that judged it was chaired and vice-chaired by people taking money from Novartis — and every one of them had declared it. Nobody hid anything. Nobody broke a rule. And the drug sailed through anyway. The conflicts didn’t derail the process, everything was just waved through because this is all completely normal. The conflicts of interest are the process.
In the end…
By now you can see the shape of this, so I’ll keep it short. NICE said yes, and NHS England signed a “world-first” deal with Novartis to roll inclisiran out to as many as 300,000 people — one of the largest medicines agreements in its history. Some of the terms are kept from us, for “commercially sensitive” reasons, so we’re told. What we do know: a generic statin costs the NHS pennies a tablet, while inclisiran’s list price is £1,900 a dose
A professor of health economics, reviewing how the deal was struck, said the NHS had been “captured as an instrument of industrial policy ”). I’d go further. Given everything we’ve just walked through — public science taken private, a drug bought on a cholesterol number, paid trialists vouching for it, conflicted committees waving it through, a regulator that won’t show its working — it is hard not to suspect this for what it looks like: a remarkably effective way to extract public money out of a national health service, at the expense of good evidence and people’s health. It is the opposite of how medical science is supposed to work.
This is one node on the Map of Distortion. There are thousands more. I’ll show you the next.